


1Department of Dermatology and 2Clinical Research Unit, Reims University Hospital, FR-51092 Reims cedex, 3Department of Dermatology, Rouen University Hospital, Rouen, 4Department of Dermatology, Limoges University Hospital, Limoges, France. E-mail: pbernard@chu-reims.fr
Accepted Nov 13, 2017; Epub ahead of print Nov 14, 2017
Autoimmune bullous dermatoses (AIBD) are rare in Western countries (1). The French Rare Diseases Reference Centre was set up in 2005, and encompasses 3 university hospital departments (Reims, Limoges and Rouen) located in 3 distinct French regions (Champagne-Ardenne, Limousin and Haute-Normandie) encompassing a total population of 3.9 million. The aim of the centre is to improve health-care, research, nursing staff and patient information, and to provide national and international recommendations. In this context, a computerized database was prospectively created in 2010, giving rise to the Regibul Register. Data from all new cases of AIBD seen in the reference centre were collected using an anonymous standardized questionnaire (CNIL authorization no. 911 0021).
Despite diagnosis and treatment advances, to date only a few studies have described the distribution and incidence of sub-epidermal AIBD (2–10, Table SI) and pemphigus (11, 12). Using data collected over a 6-year period (2010 to 2015) from the 3 reference centre sites, the aim was to describe clinical characteristics along with the initial management of included patients (primary objective), and to estimate both the distribution and standardized incidence rates of these AIBD after exclusion of patients who were not living in our 3 regions (secondary objective).
All cases of AIBD, confirmed by cutaneous direct immunofluorescence (IF) microscopy analysis, were included. The data collected were demographic information (age, sex, home location), AIBD diagnosis and date, clinical characteristics at baseline (number and location of cutaneous or mucous blisters, other skin lesions), pattern and type of immune deposits observed by direct IF microscopy analysis, serum immunopathological investigations performed at time of diagnosis including standard indirect IF or indirect IF on salt-split skin, BP180 and BP230 enzyme-linked immunosorbent assay (ELISA)s, anti-desmoglein 1 and 3 ELISAs, and the initial type of management of patients (hospital or specialized outpatients’ clinics).
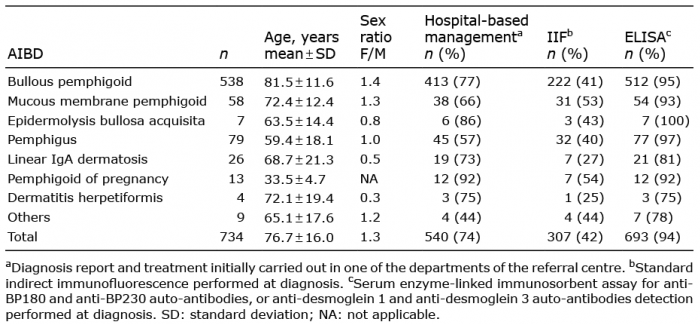
A total of 734 cases of AIBD were recorded, including 538 cases of BP (73%), 58 mucous membrane pemphigoid (MMP) (8%), 7 epidermolysis bullosa acquisita (EBA) (1%), and 79 pemphigus (11%) (54 pemphigus vulgaris (PV), 23 pemphigus foliaceus (PF)) (Table I). The number of cases recorded in each of the 3 reference centres was quite similar (240, 234 and 260, respectively) with most of patients (n = 599, 82%) living in the administrative region of the reference centre. Diagnostic and therapeutic management were initially performed at hospital in 540 cases (74%). At baseline, 253 patients with BP (47%) had extensive disease (i.e. more than 10 daily blisters) and 61 (11%) had mucosal involvement, almost exclusively oral. Within MMP patients, oral involvement was present in 37 cases (77%), ocular in 20 (42%), cutaneous in 30 (52%) and genital in 8 (17%). At diagnosis, the detection of serum autoantibodies was investigated by standard indirect IF in 307 cases (42%) and by ELISA measurement in 693 cases (94%) (Table I). Indirect IF on salt-split skin was performed at diagnosis in 504 cases of BP (94%), in 55 cases of MMP (95%) and in all cases of EBA (n = 7).
Table I. Demographic characteristics and diagnostic management of the main autoimmune bullous diseases (AIBD)
Standardized incidence rates of all AIBD, of bullous pemphigoid (BP) and of pemphigus were calculated using the distribution by age group of the French population, both in the whole population and by sex. For standardized incidences rates, only patients living in the administrative region of the reference centre (n = 599) were considered. Based on the data in the Regibul Register, the annual standardized incidence rates were 24.9 cases per million people (95% CI 22.9–26.9) for the AIBD as a whole (22.7 for females, 29.2 for males), 18.8 cases per million people (95% CI 17.1–20.5) for BP (16.6 for females, 22.4 for males) and 2.1 cases per million people (95% CI 1.6–2.7) for pemphigus (2.0 for females, 2.4 for males).
To our knowledge, the Regibul Register is the first example of a prospective computerized registry to identify all of the AIBD cases observed during diagnostic and care activities of a dedicated reference centre. Of note, all data from this register came from a prospective collection, unlike previous studies intended to describe AIBD distribution that were issued from retrospective registries (1, 3–5, 7–11, 14), apart from 2 of them dealing with small series of patients (2, 6). As expected, BP was the main AIBD subtype, accounting for almost 75% of the whole AIBD diagnosed and even more than 80% of the sub-epidermal AIBD subset. In addition, MMP and pemphigus accounted for only approximately 10% of the total AIBD. The low proportion of pemphigus within AIBD and its low incidence in the Western Europe countries were further confirmed in this study, as well as the predominant occurrence of PV over PF (11). Such a distribution of sub-epidermal AIBD and pemphigus is similar to that described in previous retrospective studies (3, 7, 10, 11, 14) and 2 prospective studies (2, 6). It is worth noting that these results are also in line with those of a recent study related to AIBD prevalence in Germany, based on the database of a major health insurance company (1). Such a concordant result demonstrates a good representativeness of the Regibul database, despite a potential negative recruitment bias for BP, the most common AIBD. In fact, it is very likely that home remoteness to the referral centre and a less extensive BP (e.g. moderate or localized), which may be treated by dermatologists outside our reference centres, represent significant negative recruitment biases. Such a bias is, however, less important than those of disease registries amalgamating information on patients with AIBD worldwide with very heterogeneous geographical origin (15). Interestingly, our present results fit with previous French studies (2, 11–13). Indeed, BP annual crude incidence in France has shown a 3-fold increase between 1995 and 2012 (7.4 and 21.7 cases per million people, respectively) (2, 13). Concomitantly, the crude annual incidence of pemphigus in France remained fairly constant, with 1.7 and 2.7 cases per million people in 1995 and 2010, respectively (11, 12).
The interest of this register, in addition to its prospective nature, is the reliability of the data collection made by expert dermatologists in AIBD from well-documented cases, as well as its ease-of-use bound to computer recording. Then, it could be profitable both for epidemiological surveillance and for AIBD recording activities bound to referral centres. In the long run, it could also be used more widely by French hospital-based dermatologists less specialized in AIBD, allowing theoretically an overall estimation of the distribution and incidence of the main AIBD at a national level. In fact, the Regibul Register represents the first step of a continuous recording of new cases of AIBD. Indeed, it will evolve in 2018 towards a large, national database, BAMARA, which will record the nominative data of the patients with rare disease visiting specialized centres, as well as the follow-up measures, which will become mandatory according to the development of the Rare Diseases Plan by the French Ministry of Health.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize